Bone expansion techniques, conceived to increase peri-implant bone volumes using the native bone of the site where the implant is to be inserted and the use of bone expanders to stabilise implants in type 3 and 4 bone structures, are well documented techniques recognised as valid and reliable by surgeons and by the literature. The critical point of these techniques is that the protocol contemplates the use of a surgical mallet to guide the instruments in creating the implant bone socket. The impact produced by the surgical mallet may cause a vertigo syndrome in patients which may also be very annoying and sometimes long-lasting.
To avoid or reduce this symptom to a very significant extent, last year Sweden & Martina introduced the Magnetic Mallet, a dynamic magnetic instrument consisting of a handpiece powered by an electronic control unit which controls the forces and times of application. The aim is to bind an adjustable shock wave, with calibrated force application time, to the handpiece of the bone expanders and to transmit this shock wave to the tips of the bone expanders.
The Magnetic Mallet produces a greater energy with elevated accelerations applied in much shorter times compared with the classic surgical mallet. In this way a plastic deformation of the bone can be induced which absorbs the whole shock wave, thus avoiding the creation of inertia affecting the rest of the cranium.
The shock waves generated using the traditional surgical mallet and using the Magnetic Mallet have been measured on natural models.
- 1) With the surgical mallet the shock wave generated was 40 Dan (Deca Newton) (40 Kg) for a time of 200 µs; much of the energy thus obtained was not exhausted in the plastic deformation of the bone, but went on to influence the whole maxillary mass;
- 2) with the Magnetic Mallet the shock wave generated was 130 Dan (130 Kg) applied for 80 µs. In this way the plastic deformation of the bone was enormously facilitated and allowed the total absorption of the energy, while the acceleration on the maxillary mass remained minimum and indeed negligible.
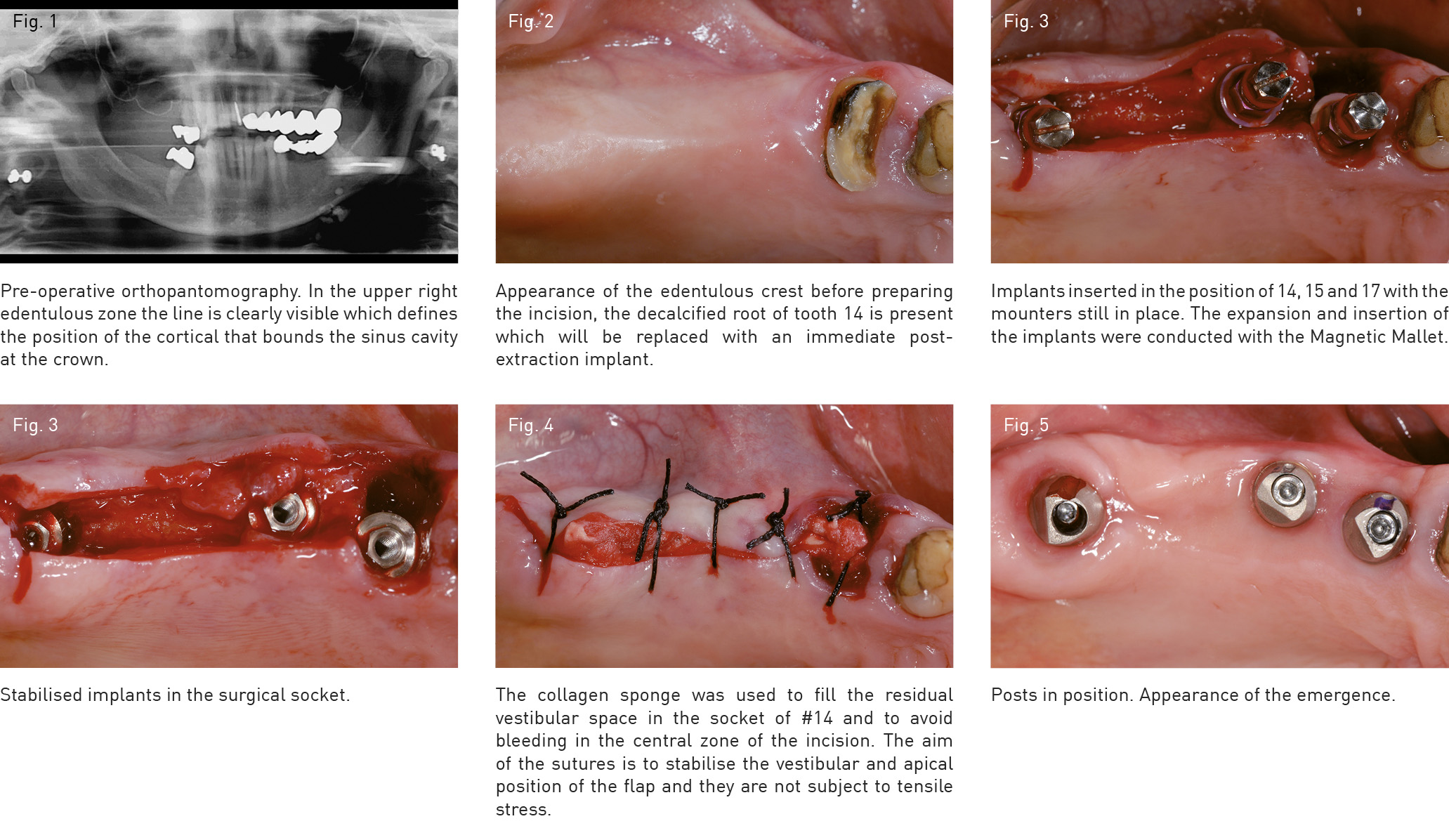
The instrument perfectly performs the function for which it was designed, that is to make the manoeuvres more acceptable for the patient when it is necessary to divide the bone structure, widening it to create an adequate surgical socket, with an adequate position and thickness of the most critical walls of the socket (namely the vestibular and the oral wall), in which to insert the implant.