












The patient, female, 55 years old, came to our observation with pain and mobility of the elements 4.4 and 4.5. A bridge was previously made on the same two elements subjected to root canal therapy and restored with posts in biomedical alloy. The patient denied recent or remote systemic disorders in her medical records and was able to sign informed consent. During the clinical evaluation, the elements resulted proved hopeless: the periapical radiograph of the element 4.4 shows an apical lesion of endodontic origin; moreover, the bridge 4.4-4.5 presented a grade 2 mobility. Given the need for prosthetic recovery, for the elimination of the present inflammatory process and the impossibility of recovery by endodontic re-treatment, in agreement with the patient both elements were extracted and replaced with two Prama implants, chosen for the particular design of the neck.
To proceed with a post-extraction insertion, the vestibular bone wall was preserved both in thickness and height during the avulsion phase. The apical bone volume permitted to insert the implant beyond the post-extraction sockets and therefore to obtain a good primary stability of the fixture after insertion. In addition to the width, also the height and the inclination of the alveolar crest and the height of the alveolar bone near the adjacent teeth allowed to proceed with a post-extraction insertion with excellent chances of success.
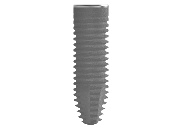
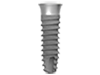
Furthermore, to have a greater control over aesthetic profiles, at the insertion time we chose Prama implant by Sweden & Martina; in fact, the convergent portion allows a submerged positioning of the implant with respect to the lingual side of the alveolus. This versatility in positioning is linked not only to the three-dimensionality of the implant neck, but also to the UTM surface finishing: the micro-thread has proved to be an ideal substrate both for hard and soft tissues.
During the 3 months after surgery, the implants were left healing with the Prama IN healing, which close on the implant neck embracing it for 0.5 mm and which help the rapid conformation of a thick and healthy mucous tunnel, characterized by a clearly visible creeping. Once the soft tissue maturation was considered complete, a definitive zirconium-ceramic screw retained bridge is made. Initially the prosthesis caused a light tissues ischemia since the emergence profiles were designed to refine the conformation initially obtained with the healing abutments. After about ten minutes soft tissues were already adapted to the new morphology and the patient didn’t report any discomfort or pain. The patient was included in a 4-month professional hygiene recall program and was subjected to oral hygiene instructions.
Follow up was performed at 3-6-12-24 months. The implants were clinically and radiographically healthy. The aesthetic aspect met our and patient’s expectations. We did not observe inflammatory processes in proximity to marginal tissues, nor bone or tissue recessions.
To proceed with a post-extraction insertion, the vestibular bone wall was preserved both in thickness and height during the avulsion phase. The apical bone volume permitted to insert the implant beyond the post-extraction sockets and therefore to obtain a good primary stability of the fixture after insertion. In addition to the width, also the height and the inclination of the alveolar crest and the height of the alveolar bone near the adjacent teeth allowed to proceed with a post-extraction insertion with excellent chances of success.
Furthermore, to have a greater control over aesthetic profiles, at the insertion time we chose Prama implant by Sweden & Martina; in fact, the convergent portion allows a submerged positioning of the implant with respect to the lingual side of the alveolus. This versatility in positioning is linked not only to the three-dimensionality of the implant neck, but also to the UTM surface finishing: the micro-thread has proved to be an ideal substrate both for hard and soft tissues.
During the 3 months after surgery, the implants were left healing with the Prama IN healing, which close on the implant neck embracing it for 0.5 mm and which help the rapid conformation of a thick and healthy mucous tunnel, characterized by a clearly visible creeping. Once the soft tissue maturation was considered complete, a definitive zirconium-ceramic screw retained bridge is made. Initially the prosthesis caused a light tissues ischemia since the emergence profiles were designed to refine the conformation initially obtained with the healing abutments. After about ten minutes soft tissues were already adapted to the new morphology and the patient didn’t report any discomfort or pain. The patient was included in a 4-month professional hygiene recall program and was subjected to oral hygiene instructions.
Follow up was performed at 3-6-12-24 months. The implants were clinically and radiographically healthy. The aesthetic aspect met our and patient’s expectations. We did not observe inflammatory processes in proximity to marginal tissues, nor bone or tissue recessions.