The perception of success in implantology does not necessarily coincide with the technical concepts involved, but sometimes this must be combined with the expectations and desires of patient. The case presented here is of a patient seeking implant rehabilitation of her lower frontal sector, although her greatest anxiety was to avoid repeating the experience of a number of implants she had been fitted with many years before, and which, although still satisfactorily functional, had become aesthetically unsightly due to the exposure of metal at the gingival margins.
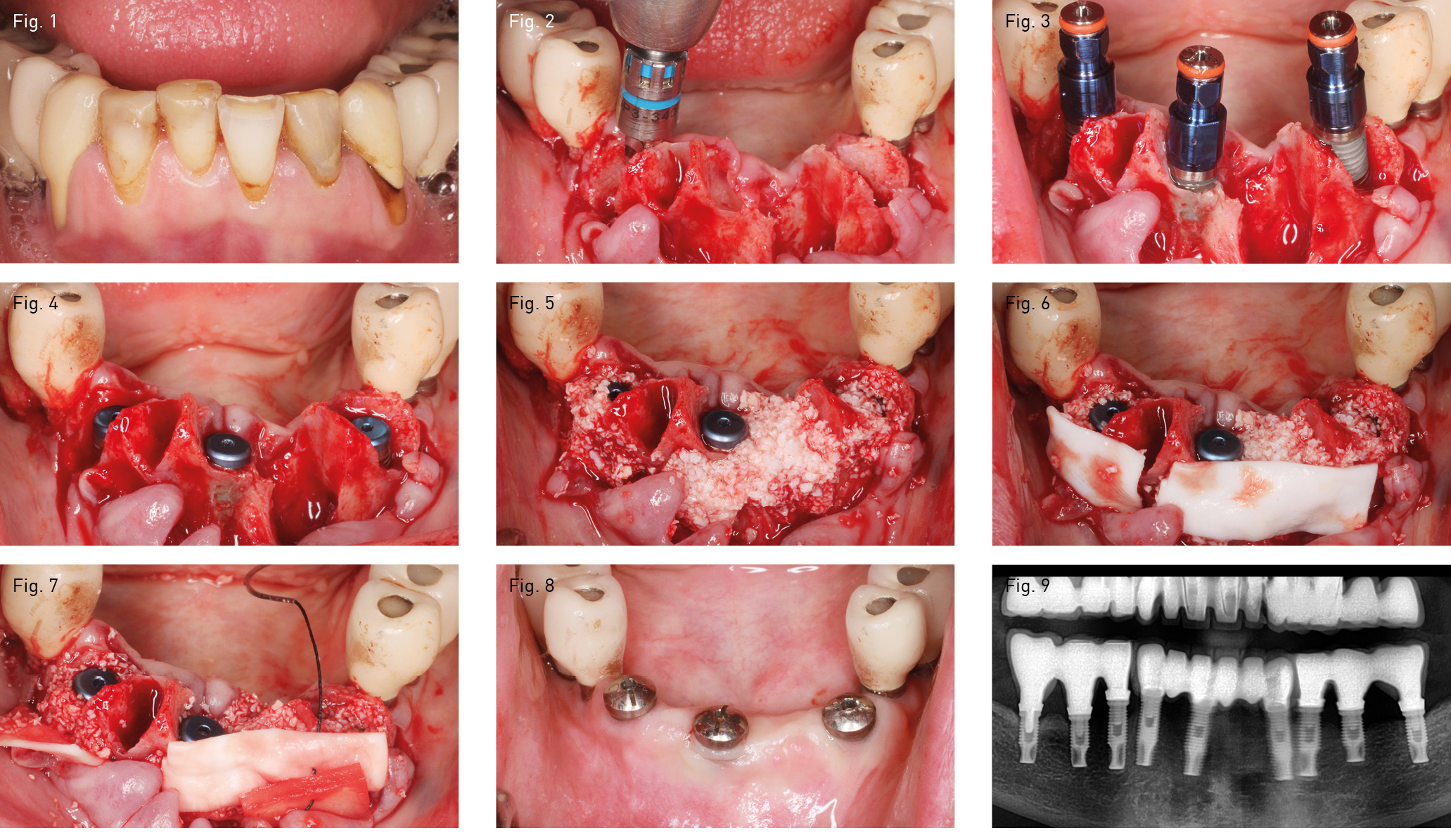
Given that case presented significant recession at the level of the canines (fig. 1), the professional challenge – apart from the obvious need for functionality – centred on successfully achieving a uniform emergence profile in the forthcoming restoration supported by implants. The teeth were extracted and the extraction sites and bone defects caused by the infective pathology were meticulously curetted.
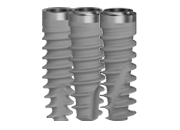
Three Sweden & Martina Outlink2 implants with external connections were fitted, with lengths 13 mm and diameter 4.10 mm (figs. 2, 3 and 4). The discrepancies between the implants and sockets and the concomitant bone defects were filled with an insert of a particulate alloplastic material, and the area was covered with resorbable collagen membranes (figs. 5 and 6). Similarly, the area of gingival recession was compensated for with a dermal matrix that was sutured together with the membrane and the coronally repositioned flap (fig. 7).
After waiting 3 months to achieve an acceptable maturation of the tissues, a screw-retained ceramic prosthesis was fitted, with gingival emergence profiles that – fortunately – the patient approved (fig. 8 and 9).