Introduction: Surgical treatment on thin alveolar crests for implants has always been a difficult task, even for the most experienced implantologists. The many surgical techniques suggested in literature may confuse clinicians to a certain degree in the choice of the correct surgical technique to be used.
The main surgical techniques found in literature can essentially be divided into two basic groups:
Split-crest techniques, which aim to divide the thin crest present into two parts to be opened out, thus creating an intraosseous bone defect delimited by the two split cortices.
Regenerative techniques, which leave the residual thin crest intact and increase the thickness of the crest with the application of a block or particulate graft, protected by a membrane or a titanium mesh.
The two therapeutic options are very different, although they often give the same clinical results.
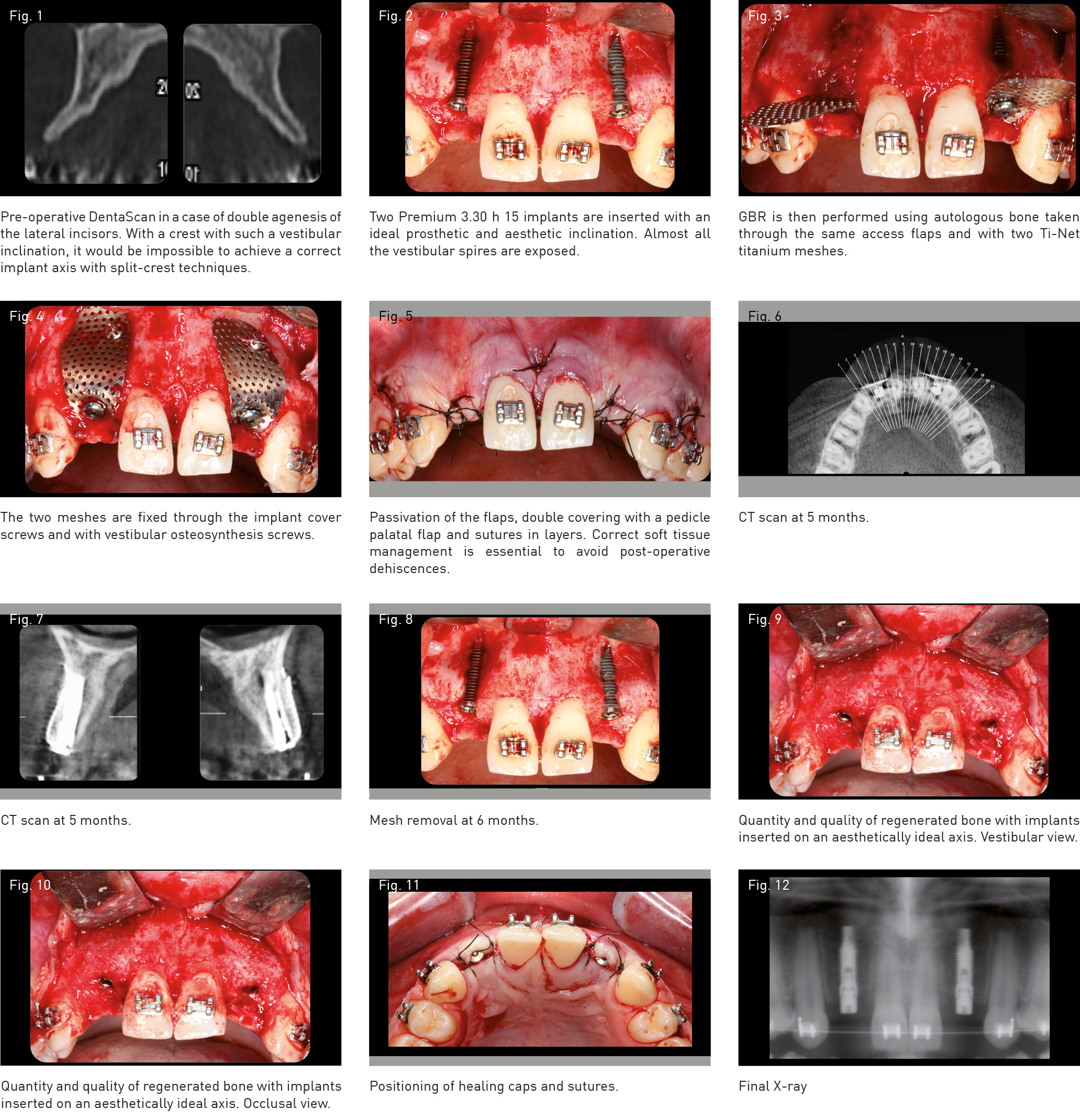
We will therefore describe an explanatory case involving bilateral thin crest at positions 12 and 22 that cannot be treated with split-crest techniques due to excessive vestibular inclination (S-shaped). Horizontal bone regeneration must therefore be performed to obtain aesthetically correct inclination for implants. For many years, in our clinical practice, titanium meshes have successfully replaced the reinforced non-resorbable membranes that we used previously. In our experience, the advantages of meshes are essentially a more stable and predictable closure of the soft tissues, due to the anchorage of these latter through the micropores of the mesh, a much greater stability and robustness of the combination of meshes, implants and stabilization screws, and a significant reduction of late exposures in comparison to membranes in Gore-Tex.
Conclusions: If used within the specific field of respective indications, both surgical techniques have shown themselves to have high predictability and high success rates, giving us the possibility of resolving even complex cases and particularly difficult crests with a single surgical operation.
In our opinion, both surgical techniques are highly operator-dependant, and correct training and frequent clinical practice seem to be fundamental for the reduction of the incidence of complications.
Of the various surgical techniques available, we choose split-crest techniques whenever we can, so as to be able to exploit the great osseogenetic capacities of two split cortices, and to reduce costs as much as possible and to avoid re-entry procedures for the patient.
Split-crest techniques must however be avoided in these cases:
if DentaScan imaging shows that the crest to be operated on is thinner than 2.5 mm;
if the crest, regardless of its thickness, is formed solely by cortical bone, a very common situation in mandibles;
if the residual crest has excessive vestibular inclination, which would be accentuated by the split crest.
In all these situations, we opt for guided bone reconstruction using titanium meshes.
The reconstruction technique using meshes must also however be studied and prepared even when the choice is made for a split-crest technique, given that it allows the operation to be terminated successfully even in case of a massive fracture of the vestibular cortex during split manoeuvres (rescue technique).
By carefully choosing the surgical technique best indicated for the single clinical case in question, even particularly complex clinical cases can be resolved predictably and with high success rates.