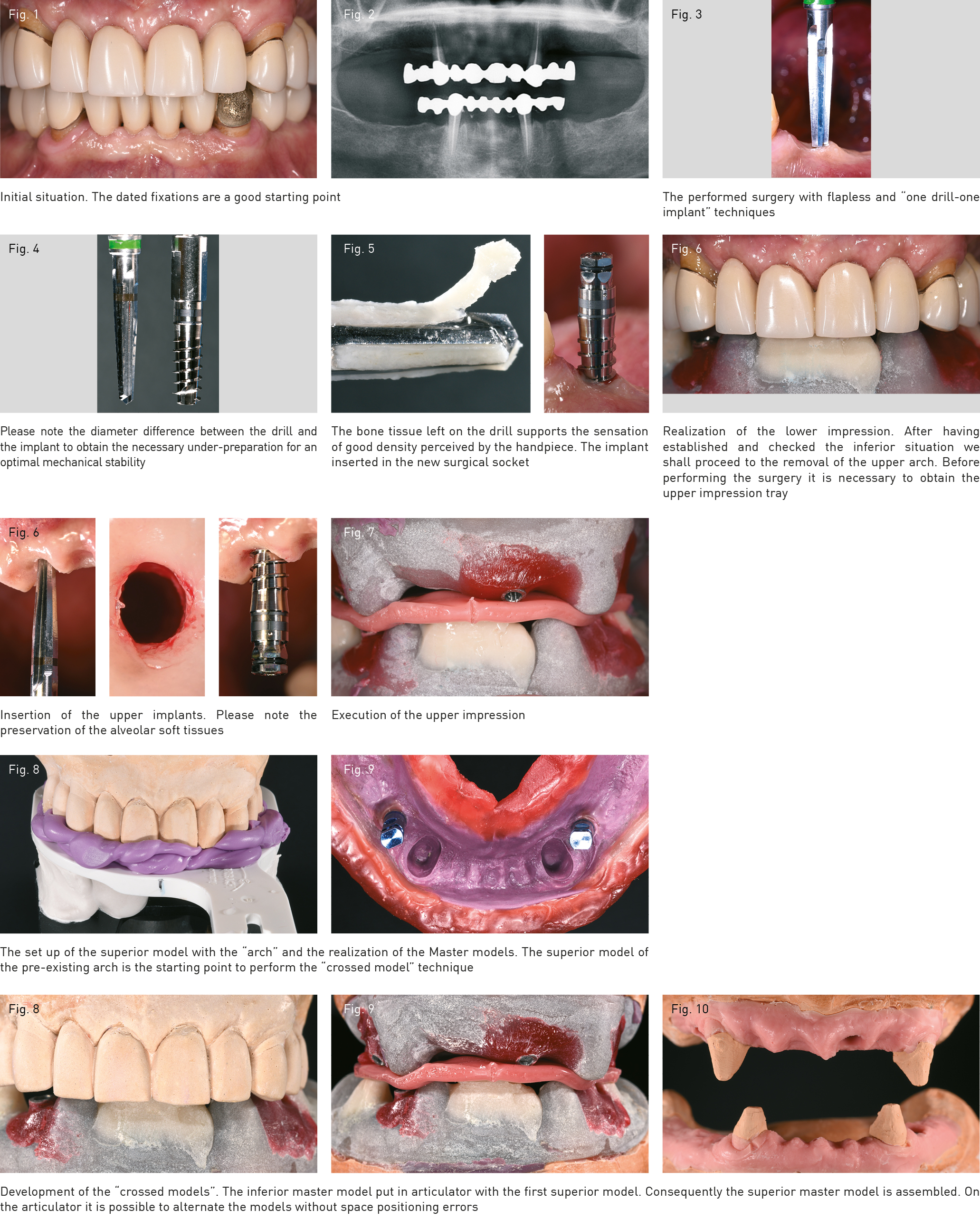
Mr. Luigi, a long-standing patient, who had for about twenty years a fixation in gold resin supported by his canines which were oscillating by now and could not be without teeth for professional reasons. The ideal treatment plans or, if you like, the “traditional” ones to correctly rehabilitate the situation collided with the expectations just described. The bimaxillary prosthetization uses the masks obtained from the diagnostic set ups which provide a reliable forecast of the finalization and are the guides for the recording steps and the prosthetic development. In this case they could not be used because the surgery considered the extraction of the canines only after the insertion of the completed Toronto. The old fixations of Mr. Luigi, from which we can obtain a lot of information after an accurate analysis, become the guide lines for our rehabilitation based on the crossed models concept, which allow us to assemble different models of the same mouth on the articulator without space errors. The partially scarped resins suggest a control and a lift of the Vertical Dimension which encountered with the description of an excellent sense of well-being of the patient. It has been decided to keep the usual parameters and therefore record the height which must be observed in every procedure. The registration of the facial arch occurs directly on the old upper arch. After the removal of the lower arch, with the impression in alginate an immediate impression tray was manufactured very adhesively in order to not generate obstructions; from the fixation model it would not have been possible to obtain it so accurate. In the meantime the surgery of the inferior arch with the insertion of two Syra Machined Implants (Sweden & Martina) with the insertion torque > 80 Ncm was performed. The recording of the inferior impression is realized with titanium sleeves properly shorten using the stent for the height. After the relining, the sleeves are fixed with self-polymerizing resin following the salt and pepper technique to control the retraction and a recording with a thin layer of wax between the lower impression tray and the upper arch is performed before this is removed. While the individual impression tray is being manufactured the surgery of the upper arch with the insertion of three Syra machined implants is performed. The recording of the impression occurs with the same technique of the inferior arch. In this phase it is important to not influence the Vertical Dimension which at the control with the stent, including the thicknessof the chewing wax, is still corrected. In the laboratory the crossed model procedure is performed, the superior model of the old fixations with the facial arch is assembled in the articulator, and subsequently the inferior master model is assembled and the superior master consequent to the inferior master. The starting point for each next step is the first model on which the information of the arch, the images and the indications taken in the recording phase the occlusal plan, the vertical and horizontal lines corrections are applied with wax directly on the model. In the realization phase this simple way to set the macrogeography of the rehabilitation can be subject to modifications and adaptions to find a better compromise between the implant position, crestal relation and occlusal scheme. Therefore we begin with a remarkable quantity of information obtained in one single appointment in which the surgeries and all the necessary recordings are performed. The patient, during the manufacturing of the new prosthesis, is living his social and professional life normally with his replaced old arches in gold resin. We can proceed to realize the structures with the crossed models and a small silicone mask, which give us a reasonable determination of the volumes.