CLINICAL CASE
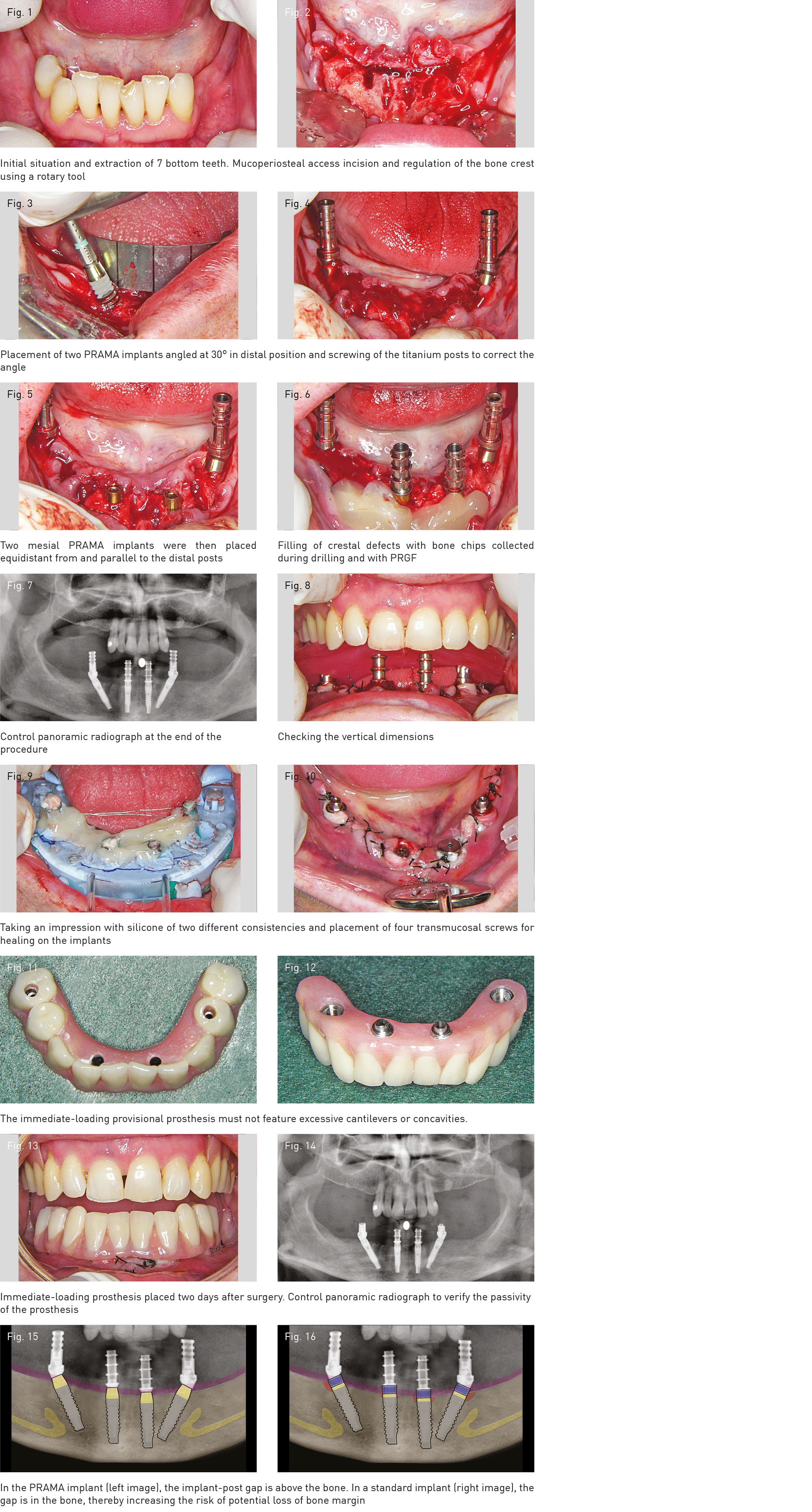
A 63-year old female patient with no prior medical history of interest presented advanced periodontitis of the lower-anterior elements and the posterior edentulous areas with significant atrophy of the crest thickness. After appropriate pre-operative planning, 7 anterior elements were extracted before lifting the full-thickness mucoperiosteal flap in the anterior area (with central and lateral release), thereby allowing good access to the inter-mental foramen region, where the All-on-Four specific technique was initiated, thus regulating the crestal profile using a rotary tool, removing the bone peaks from post-extraction sockets, before levelling the vertical bone surface to ensure that the four implants are on the same occlusal plane. A central bone perforation of 2 mm in diameter and 10 mm of depth was then made, aligned with the midline of the face, in order to place the shank of the All-on-Four specific curved metal guide (manufactured by Nobel Biocare). This has vertical incisions that enable distal implants to be placed at an angle of approximately 30° while keeping the tongue away from the operating area. With the aforementioned guide in position, the emergence areas of the mental nerve (for appropriate intra-operative control) were marked on the bone with a sterile surgical pencil, as well as the 30° surgical drilling angle, to make it much easier to check the correct inclination of the drills, bone taps and placement of the two PRAMA 3.80 x 15.00 mm distal angled implants. Intermediate drilling was also performed (using conical drill bits) as an additional precautionary measure to generate minimum placement torque of 35-45 Ncm and for deeper placement of the golden neck of the distal implant to not leave any mesially exposed threads. Once the two distal angled implants were inserted, the angled P.A.D. abutments (code A-PAD-AA330-303) were positioned to correct the angle of the non-parallel screw retained prosthesis (screwing torque 20-25 Ncm). The corresponding rotating titanium sleeve (code PAD-CT) was then screw retained onto the P.A.D., with a screwing torque of 20-25 Ncm. These two components tightened onto the tilted Prama implant fully corrected the disparallelism and minimised the use of distal cantilever bridges of the pending immediate-loading prosthetic. The sites of two mesial implants were then prepared as equidistant from, and parallel to each other and the two distal P.A.D. abutments as possible. The same procedure was performed to place another two PRAMA 3.80 x 13.00 mm implants in this position with a minimum screwing torque of 35-45 Ncm, with intermediate drilling using conical drill bits. Two non-engaging, temporary, straight titanium posts were tightened directly into these two central implants (code A-MPSA-330), without the need for any intermediate abutment thanks to the morphology of the large transmucosal portion of the PRAMA implant.
Crestal defects were then filled in with PRGF mixed with bone chips collected during drilling and the flap was sutured, leaving the four titanium posts exposed. A control panoramic radiograph was then performed, which brought the surgical phase of the All-on-Four procedure to a close. The prosthetic phase then began, using the occlusal height of the four posts to conduct an occlusion test with a silicone rim, verifying the vertical dimensions and the mandibular jaw position in terms of centric relation. Impressions of the four titanium posts were then taken using silicone of two different consistencies and a perforated dental impression tray. These posts were fixed off the tray with orthodontic metal ligatures coated in light-curing composite resin. A solid and reliable open tray impression was thus obtained, recording the position of the four implants and the morphology of the soft tissues. Four transmucosal screws for healing were then placed on the PRAMA implants and the patient was given an appointment two days later to place the new screw retained provisional prosthesis. In this case, prescribed prophylaxis began the day before the surgery and consisted of Augmentine Plus every eight hours for eight days, Ibuprofen every eight hours for five days, Fortecortin one vial per day for four days and Chlorhexidine 0.12% mouthwash every eight hours for 15 days. Production of the prosthesis began immediately, first from the impression taken previously and then working with a gypsum model, removing irregularities of the gingival margin caused by the sutures to produce a smooth and homogeneous gypsum model. From this moment, the prosthesis is made, first through the impression taken in advance, then preparing the model, eliminating the irregularities of the gingival margin due to sutures, thus obtaining a more refined reproduction of the tissues and gaining more hygiene in the resin of the prosthesis manufactured by the laboratory. Two days after the surgery, the patient returned to the clinic for placement of the new provisional prosthesis. Intraoral and extraoral outcome and appearance were completely favourable.
It was checked during the placement phase that the prosthesis did not feature excessive cantilevers and that there were no cavities or non-hygienic spaces between the base and the tissues. The transmucosal screws were then removed and the prosthesis tightened into place. This procedure was greatly simplified thanks to the PRAMA implants, which feature a large transmucosal portion hardly embedded in the gums to facilitate clinical manoeuvres. The procedure was concluded with an orthopantomography to ensure appropriate passivation of the prosthesis on the implants as well as correct occlusion and aesthetic appearance. The sutures were removed after two weeks and a monthly follow-up plan was scheduled for the next five to six months. The planning and production of the final prosthesis also began. The provisional prosthesis did not have to be removed throughout this period.
We have therefore had a detailed insight into the All-on-4 immediate-loading implant-prosthetic rehabilitation technique and can conclude that it is undoubtedly an effective and accessible method to achieve our key objectives for a fixed prosthesis on implants, given its simplicity, safety, affordability and comfort. Furthermore, we have also been able to verify that using PRAMA implants in this type of treatment seems to offer a number of advantages deriving from the morphology of the implant itself and its large machined transmucosal section, as follows: unlike with other implants, with the PRAMA implant there is no need to excessively drill into the bone crest for the angled implant to distally embed its occlusal plane into the bone so as to not leave any mesially exposed threads. This both preserves bone and, more significantly, prevents the risk of “cratering” bone defects deriving from the transepithelial implant-abutment joining gap. There is also no need to use transmucosal intermediate abutments in the two straight mesial implants, into which the titanium temporary post is screwed directly. This greatly facilitates intraoral clinical manoeuvres and requires fewer screws and prosthetic components. Exposure of the machined neck of the implant due to the physiological gingival recession that takes place during the post-operative tissue remodelling process does not pose a problem for the final prosthesis as the coronal portion of the PRAMA has no shoulder or chamfer. It can also freely adapt to the margin of the prosthesis by means of the B.O.P.T. technique at any level of its coronal hyperbolic portion. In conclusion, on the basis of the above clinical case, the PRAMA implant seems to offer a number of interesting advantages when used in combination with the All-on-Four technique. However, it is important to bear in mind that the exceptional validity of this pairing can only be judged based on the medium-and long-term outcomes of clinical cases and studies.