Ninety-three percent of 4 to 6 year-olds are candidates for this preventive orthodontic procedure.2,3 The appliance can eliminate buck teeth (overjet) of any severity, crowding up to 7mm in the deciduous dentition as the permanent incisors erupt (equivalent to 4mm of permanent crowding), overbite (where the upper front teeth cover part or all of the lower front teeth when the child closes his/her jaws), and open-bite (stops thumb-sucking - 20%). This can be achieved by wearing the NG only while sleeping.
About 4 out of every 5 children will experience one or more dental problems, such as crowding, rotated teeth, overjet and overbite as the adult teeth begin to come into the mouth. By using the natural forces of eruption, the NG appliance can guide adult front teeth into their proper positions and eliminate crowding, rotations, overjet, overbites and open-bites. Once the child’s adult teeth have been guided into their proper positions by the appliance and have fully erupted, adult periodontal fibers form around the roots and lock the permanent teeth into the correct occlusion. This prevents these new teeth from relapsing. Also, relapse is frequently avoided because sufficient facial and jaw growth is present when the NG procedure is started at this early age, which helps to insure that the correction will remain stable in the future. Postponing treatment until a later age (11 to 14 years), when most of the adult teeth have fully erupted and the fibers have locked in the malocclusion, results in about 75% relapse according to research. At this later age, there is also less growth left for the child, which is necessary to stabilize most orthodontic corrections, particularly overbite and overjet.
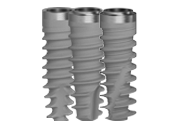
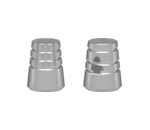
During the first years of school, those children that appear to be “different” because of some aspect of their physical appearance may become a target for teasing or other abuse, which can decrease their developing self-confidence. The NG preventive treatment can help to give the child a normal dental appearance and improve his or her profile, smile, and self-confidence.The NG technique usually involves 2 appliances. The first, the “C” series comes in 11 prefabricated sizes, shown in Fig. 1. The second appliance, used after about 5 months is called the “G” series (Fig. 2) and comes in 13 prefabricated sizes. Both appliances are used only passively while sleeping. The appliance sizes are measured with a small measuring guide.
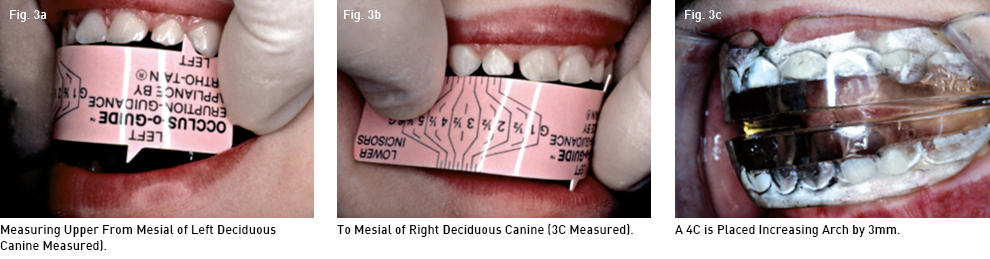
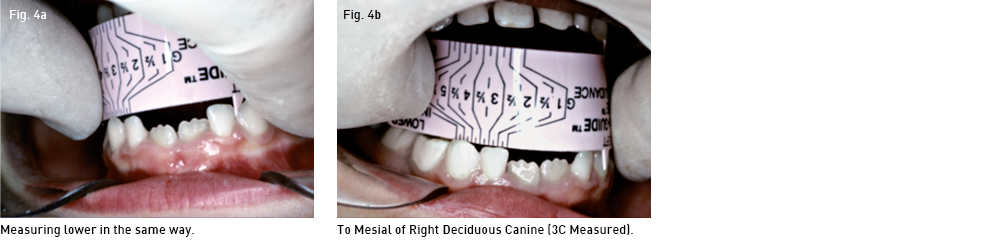
Measurement - The most usual measurement is from the mesial of the upper left deciduous canine to the mesial of the canine on the other side (Fig 3 a,b,c). If the upper arch is difficult to measure accurately due to flared incisors, or missing or unerupted teeth, then the lower arch from canine to canine can be used with the other side of the ruler (Fig 4a,b). A slightly larger NG is used, than is actually measured, and is usually ½ to 1 full size larger when additional space is required for the permanent lower central incisors to erupt straight. This first appliance is usually a “C” series Nite-Guide. When the lower laterals erupt through tissue, a second appliance is then used. It is usually a “G” series and most often at lease two full sizes larger than the first appliance, and is the last one used. It serves also as the retainer until about 12 years of age when the patient is dismissed. Only nighttime passive wear is necessary. The reason for this is to take advantage of the normal and expected developing arch circumference increase as the central and lateral incisors approach the tissue and enter the arch, which typically increases 3.5mm when the teeth erupt straight. It is extremely important to anticipate this increase as these teeth erupt, so as to maximize the increase rather than restrict it, especially when crowding is anticipated. Very rarely are the permanent incisors smaller than the available space between the deciduous canines, but when this does occur, it is important to recognize it so that the NG procedure can be reversed. This would be done by beginning with a NG that is smaller than the existing space so as to close the excess interproximal spaces.
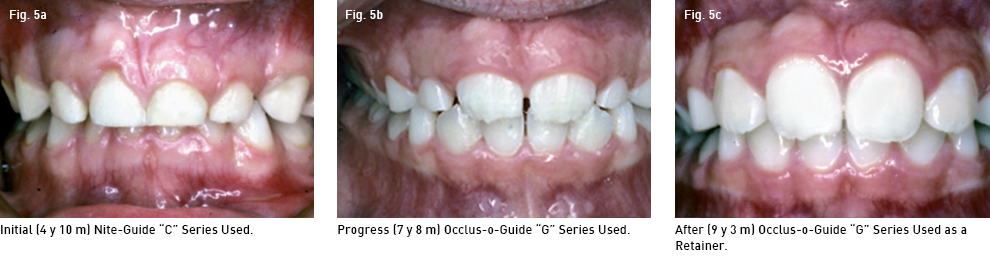
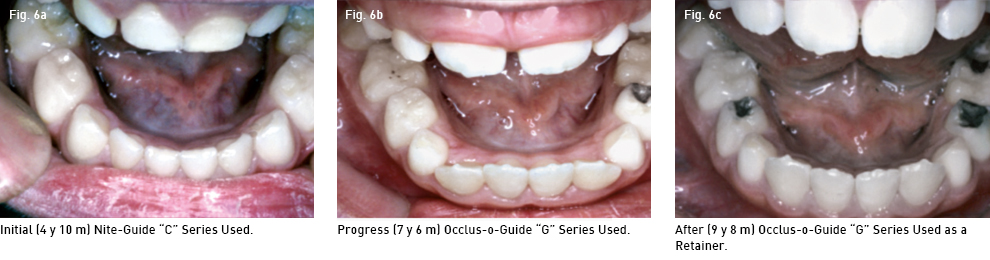
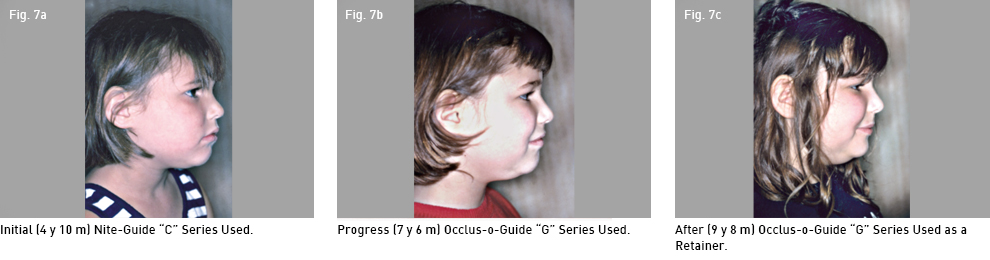
A typical case is shown (Fig. 5, 6, 7) with an initial deciduous overbite of 4.25mm (Fig 5a), which is destined to increase by 2mm as the adult incisors erupt to become a 6.25mm permanent overbite. The first appliance used was a Nite-Guide “C” series #3C (while a measurement from the mesial of the left canine to the other side indicated a #2). The #3 will increase the incisal arch by 1.6mm. The appliance stayed in all night while sleeping after 5 months. The patient only wore the appliances while sleeping throughout the treatment and retention period. The appliance was increased to a “3.5 G” as the lower adult laterals began to erupt. Figures 5b, 6b and 7b indicate the progress after the Occlus-o-Guide (3.5 G) had been worn after the lower permanent laterals broke tissue. Figure 5c, 6c and 7c show the patient in retention after 10 months. Note the overbite and facial profile improvements. The overbite improved 3.75mm and the overjet improved 3.5mm. The ideal final result in a female (prior to the start of puberty) should be 1.5mm of overbite and overjet, which this patient has achieved. A male should end with a 2mm overbite and overjet. This insures that future pubertal growth will not become a problem.
The very slightly crowded lower deciduous incisal segment (fig 6a) indicated an 80-100% chance of developing lower adult incisal crowding. After about 5 months from the start, a “G” series appliance replaces the initial appliance and is typically 3 half sizes larger in anticipated crowded cases. This is usually the final appliance used. It is worn each night until the upper laterals are fully erupted for 6 months. It is then used one night per week until the adult canines and premolars break tissue. The appliance should then be worn every night until the permanent second molars are fully erupted. The patient is then dismissed. The patient is seen about every 2 months for the first 2 to 3 appointments and then at 4 to 6 month intervals until the upper laterals are in place for 6 months. The patient is then seen every 6 months until dismissal. Total chair time is about 3 hours and the average fee is about 1/3 to 1/2 of a total fixed orthodontic 2-year fee. A summary review of recently published research on this technique by Keski-Nisula et al follow3,4. As well as some unpublished research by the author.